Il diabetico anziano. Gestione condivisa (Italian Edition)
Contents:
Stassen to the Commission. Erdogan's in-house ideologue states that: Right to education in the Transnistria region. Risulta alla Commissione, anch'essa informalmente rappresentata a tale riunione dallo stesso Presidente Barroso, se fra gli argomenti trattati fosse compreso lo stato della procedura di adesione della Turchia all'Unione europea e a quali risultati si sia addivenuti in merito?
La costruzione del terzo aeroporto di Istanbul deve rispettare il patrimonio boschivo. A seguito del ricorso di un gruppo di abitanti, che hanno denunciato il grave impatto del progetto sulla natura e l'ingente inquinamento elettromagnetico nei lavori del terzo aeroporto della megalopoli del Bosforo, il tribunale di Istanbul ne ha ordinato la sospensione.
La corte ha disposto una nuova perizia sull'impatto ambientale. As a result, the Court of Istanbul has ordered the work to be suspended and commissioned a new environmental impact study. How does the Commission intend to keep watch, so that completion of this work does not entail the destruction of whole swathes of forest assets? The Commission is aware of the issue raised by the Honourable Member. As a result several large infrastructure projects, including the new airport in Istanbul have been excluded from the environmental impact assessment.
The Commission will continue raising its concerns with the Turkish authorities at all appropriate fora, including the upcoming EU-Turkey Association Committee. Secondo alcune fonti Tareq al-Hashemi sarebbe stato accolto in Turchia. L'onorevole deputato fa riferimento a una questione bilaterale tra la Turchia e l'Iraq. In generale, l'Unione europea segue da vicino le relazioni tra i due paesi. Le relazioni della Turchia con il governo regionale curdo KRG a Erbil hanno continuato a migliorare negli ultimi anni. The charge against him was crimes against humanity, which he allegedly committed with his death squads.
According to some sources, Tareq al-Hashemi has been welcomed in Turkey. The issue to which the Honourable Member is referring to is a bilateral issue between Turkey and Iraq. In this context, the recent rapprochement and high level visits between Ankara and Baghdad are a welcome development that could help strengthen regional stability. Emergenza rifiuti a Roma e nel Lazio: Dopo la chiusura della discarica di Malagrotta, la situazione di emergenza rifiuti a Roma e nella Regione Lazio continua a destare preoccupazione.
In particolare, appare critica la situazione venutasi a creare dopo la chiusura della discarica di Malagrotta nel mese di ottobre Risulta che parte dei rifiuti di Roma Capitale sia stata trattata fuori ATO presso l'impianto TMB di Casale Bussi e che una parte degli scarti di lavorazione sia stata smaltita presso la discarica di Monterazzano. Entrambi gli impianti insistono sul territorio del Comune di Viterbo. Negli ultimi due anni la Commissione ha seguito da vicino l'attuazione delle misure di gestione dei rifiuti nella regione Lazio. After the closure of the Malagrotta waste disposal site, the waste emergency in Rome and the Lazio region continues to arouse concern.
As yet, no sites suitable for the disposal of waste from Rome and the numerous local authorities in Rome Province have been identified, which constitutes a situation of grave criticality in terms of urban waste management. The Cupinoro disposal site, administered by Bracciano Ambiente S.
In full consideration of the above, can the Commission answer the following questions:. As a result of this closure, some of the waste generated by the city of Rome is now being treated outside the Optimal Territorial Area OTA at the MBT plant in Casale Bussi, and a percentage of its industrial waste is being disposed of at the Monterazzano landfill site. Both facilities are placing enormous strain on the municipality of Viterbo. Is the Commission aware that the citizens living in the affected regions have been completely left out of any decision-making processes, since they have neither been involved in drawing up the time frames, procedures and documents relating to the possible expansion of the site, nor even been informed of them?
Over the last two years, the Commission has been closely monitoring the waste management measures implemented in the Lazio region. The latest developments respond to the need to treat waste before being landfilled at the available sites of Casale and Monterazzano, respectively, and to the shortage of alternatives to landfilling in the city of Rome following the closure of the Malagrotta landfill. L'articolo 2, paragrafo 1, dello stesso regolamento specifica quanto segue: Per quanto riguarda l'indagine EU-SILC statistiche europee relative al reddito e alle condizioni di vita e con riferimento alla stessa risposta alle interrogazioni 4 e 5 nella replica del , Eurostat non dispone di elementi che lo inducano a ritenere che l'istituto statistico nazionale italiano non abbia rispettato i requisiti stabiliti dal regolamento CE n.
Can the Commission indicate whether it considers that ISTAT has complied with the standards and regulations referred to above and professional ethics in the light of the fact that it has: They shall be the most recent official forecasts, taking into account the most recent budgetary decisions and economic developments and prospects. The field work date is correctly recorded in the validated data file and the quality report documents the evolution of the methodology used and of the imputation procedures.
Minaccia radioattiva alle porte di Taranto. Un impegno da parte di tutte le istituzioni italiane ed europee a breve termine potrebbe essere fondamentale per evitare che accadano incidenti imprevisti, quali esplosioni ed incendi, che comprometterebbero la salute di chi popola quel territorio.
Il tipo di rifiuti a cui fa riferimento l'onorevole parlamentare dovrebbe essere preso in considerazione nel programma nazionale italiano. Inspectors from the Italian Forest Corps inspected and searched the building in Since then there has been no changes for the better in the situation. It has been impossible to obtain accurate data about the drums, because of the way they have been positioned and the inevitable deterioration which they have suffered in the course of time. As time went by, the company which owned the site received drums from all over Italy. It went bankrupt after a long lawsuit, leaving the local authority to meet the costs of the clean-up.
Difficulties arise from an insufficient budget. It is important to take initiatives to secure the building and stop the drums deteriorating. Action must be assessed to reduce the stock present in the shed, and spread it to other parts of the country. A commitment by all the institutions of Italy and Europe could be essential, in the short term, to prevent unforeseen accidents occurring, such as explosions and fires, which would put public health at risk in the area.
Is the Commission already aware of the situation affecting the Taranto area? Can it consider the possibility of sending a team of experts to count the drums in detail and check their contents? Is it aware of the great importance of making the building secure, and of the damage which possible accidents might cause to public health and to the environment? The Commission is aware of reports in the press concerning the facility. It has established contacts with the Italian authorities and requested further information from them.
Once the Commission is in possession of sufficient and reliable information, it will decide on the possible actions to be taken. This programme has to be adequately financed and has to include inventories of all relevant waste.
The directive also establishes the ultimate responsibility of the Member States for the safe management of all radioactive waste generated in their territories. The Commission is currently checking that Member States have fully transposed the directive into national legislation. The type of waste that the Honourable Member is referring to is expected to be taken into account in the Italian national programme. We, the undersigned, ask the Commission to ensure that its representation in Romania also use Hungarian in its communications.
Its representation in Bucharest currently has no Hungarian-language media or political monitoring, and Hungarian is absent from its communications. We represent the 1. The problem damages the interests not only of the Hungarian community in Romania. The Commission must not maintain a situation whereby it neither provides information to nor monitors directly the media channels in a community which has more members than some Member States have inhabitants. These countries have their own Commission representations.
There are a number of instances of the Commission making a commitment through its representations to ethnic or minority communities in certain Member States — in Barcelona, for example, communication is in Catalan. In a number of cases the number of people in the communities in question is far lower than the number of Hungarians in Romania: The Hungarian community in Romania is entitled to information and monitoring political information at the same level and of the same quality as Romanian native speakers and the Romanian-language media.
European Commission Representations in Member States communicate in the official languages of the country in which they are based. In this case, the only official language is Romanian, as per the Constitution of Romania. In countries where minority languages have been recognised as official languages, the Commission communicates also in these languages as well. Moreover, the Commission Representation in Romania includes among its officials a member of the Hungarian community.
In reference to your question about communication with the Hungarian language media, we would inform you that the Commission Representation in Romania monitors mostly national level media outlets. She is also maintaining close diplomatic engagement with international partners, particularly the Arab League. The SPP will further develop the existing rich bilateral relations between Europe and each party and also build a triangular partnership between Israelis, Europeans and Palestinians.
Although the Agenda refers to various different kinds of vulnerable children, those living in institutions are not one of the groups. Managing child social assistance and welfare is the competence of the Member States, but can the Commission state what plans it has to help this category of underprivileged children? The Commission is strongly committed to the protection of all children and young people in vulnerable situations.
The Commission, together with the successor of the Ad Hoc Expert Group on the Transition from Institutional to Community-based Care, has been organising national seminars in the Member States to support the programming of ESI Funds actions promoting effective transition to community-based living, based on a toolkit developed for this purpose. The shift from institutional to community-based care is now part of the new European Structural and Investment Funds legislative package. The Commission expects powerful measures in this field in the programming documents for The European Regional Development Fund should support the shift to community-based care through investments in social, health, housing and education infrastructure.
Finally, the Commission in cooperation with Member States is working in ways to improve the collection of data on people living in institutions. The Commission expects that information on the size and demographic characteristics of the population living in institutions will be available from the results of the EU Population and Housing Censuses, which will be available later in EUR , der er underlagt Kommissionens direkte kontrol.
I am aware that Commissioner Hahn's spokesperson, Shirin Wheeler, has stated that the Commission is willing to launch an investigation into the specific cases concerned. Is the Commission carrying out checks as to whether firms are making improper use of EU funding in order to relocate jobs from one Member State to another?
If so, how are such checks carried out? Can the Commission give an assurance that there have been no similar instances where monies have been improperly used? If the Commission is unable to give such an assurance, does it intend to carry out an investigation into the extent of improper use of EU monies?
What new measures will the Commission take to put an end to this type of improper use of EU monies? The Commission does not support the use of EU Structural Funds in a way that would encourage or facilitate the relocation of services or production to another Member State. In accordance with the shared management principle, national or regional management authorities are ultimately responsible for ensuring that no prohibited relocation takes place. Whenever the Commission is made aware of a potential case of relocation involving cohesion policy support, it requires Member States to investigate.
If the relevant rules have not been followed, the Commission ensures that any funding provided is recovered. In Spain the current situation of crisis and privatisation has caused a sharp rise in the number of people having their water supply cut off for non-payment. Spain does not have official data on the huge phenomenon of water cut-offs, because water supplies are local services and each town and village administers them in their own way. Some towns, such as Medina Sidonia in Cadiz, fifty or so villages in Huelva, whose supplies are managed by the public company Giahsa, Zaragoza and El Prat de Llobregat in Barcelona, have decided not to cut off the water supplies of people who are unable to pay.
Was the Commission aware of the number of water supply cut-offs that are carried out in Spain? Does the Commission consider that there should be a register of official data for water cut-offs in Spain? Does the Commission consider that the water supplies of people who cannot pay should not be cut off? Does the Commission consider that access to drinking water and sanitation ought to be a human right, as recognised by the United Nations? The Commission is aware of the situation in Spain. The Commission believes that measures to safeguard disadvantaged people have become all the more important given the increase in water-poverty issues during the economic crisis and the inability of some people to pay their water bills.
It is national authorities in the Member States who are competent for taking concrete support measures safeguarding disadvantaged people and tackling water-poverty issues e. The Republic of Cyprus, as part of the memorandum of understanding with the Troika, is pushing for the adoption of a special bill on the privatisation of state organisations, including in the areas of telecommunications, electricity and ports.
The bill has encountered stiff resistance from workers and the political parties. One of the objections to the bill is that it fails to ensure the continuation of employment for, and the income and the pension rights of, workers — rights which, it should be noted, are enshrined in the Constitution of the Republic of Cyprus, since employees in these organisations have a status equivalent to that of civil servants.
Are there any are good and commonly accepted practices adopted in other cases that could also be applied in Cyprus? How can it help solve this problem and what does it recommend that the government of Cyprus do? Each Member State has its own legal framework for privatisation and for the treatment of the employees of organisations moving out of public ownership. For ease of reference, the article reads as follows: The EU's trade and investment agreements represent instruments of the common commercial policy, which pursue commercial policy objectives as its main goal.
Only one country is forecast to experience a limited period of negative inflation Greece: In addition to the fading out of some temporary factors and the continued downward trend in commodity prices, low projected inflation in the euro area reflects weak demand in the current cyclical phase, reinforced by relative price adjustments. Given the gradually strengthening recovery, the increase in confidence and the ongoing efforts to improve the health of the banking system, the risk of outright deflation in the euro area as a whole seems low.
In particular, while a rebalancing of German economic growth implying a further strengthening of domestic demand would primarily be in the interest of Germany itself, it would entail the additional benefit of providing an impetus to demand in the euro area. While relative price changes remain an important element in euro area countries' adjustment process, a further strengthening of German domestic demand would thus help address one of the factors underlying the current weak inflation trends in the euro area. EU membership requires, amongst other criteria, that the candidate country ensures the existence of a functioning market economy as well as the capacity to cope with competitive pressure and market forces within the Union.
The Commission considers Turkey a functioning market economy. An estimate of the financial implications would not be meaningful at this point. Modifying that Protocol would be a matter for the Member States, not for the Council. It is thus not for the Council to comment on the issue raised in the question. Hoe beoordeelt u het feit dat kinderarbeid en andere misstanden in de Indiase tapijtindustrie al ruim twintig jaar geleden uitvoerig in de publiciteit kwamen, dat sindsdien een aantal vrijwillige initiatieven is ondernomen maar dat de in het rapport beschreven situatie van tapijtarbeiders nog steeds ronduit dramatisch is en voor het overgrote deel bestaat uit gedwongen arbeid en kinderarbeid onder zeer ongezonde arbeidsomstandigheden en tegen extreem lage lonen?
Bent u bereid onderzoek te laten doen naar de betrokkenheid van in Europa actieve tapijtimporteurs en verkopers bij slavernij en kinderarbeid in de Indiase tapijtindustrie, waaronder de in het rapport genoemde bedrijven IKEA en Wal-Mart? Welke maatregelen gaat u nemen om er voor te zorgen dat de Indiase tapijten die op de Europese markt worden verkocht zonder slavernij en kinderarbeid zijn gemaakt?
Bent u bereid bij de Indiase regering aan te dringen op effectieve actie tegen slavernij en kinderarbeid in de tapijtindustrie en samen activiteiten daartegen te ondernemen? In het werkdocument van de diensten van de Commissie uit betreffende handel en de ergste vormen van kinderarbeid wordt de link tussen internationale handel en de ergste vormen van kinderarbeid nader onderzocht. Het is belangrijk dat een overkoepelende aanpak wordt nagestreefd die de diepere oorzaken van kinderarbeid aanpakt, zoals armoedebestrijding, toegang tot onderwijs, sociale bescherming enz.
De EU is een sterke voorstander van de ratificatie en uitvoering van de fundamentele verdragen van de Internationale Arbeidsorganisatie IAO , waaronder de uitbanning van slavernij en kinderarbeid. De Commissie bedankt de geachte Parlementsleden voor het onder de aandacht brengen van een recente studie over arbeidspraktijken, meer bepaald in India's handgemaakte-tapijtindustrie.
Gezien de al verrichte en lopende werkzaamheden, waaronder documenten van de Commissie, is de Commissie niet voornemens om een nieuwe studie te verrichten die specifiek gericht is op de sector en het land in kwestie. Will the Commission order research into ways in which carpet importers and vendors operating in Europe are involved in slavery and child labour in the Indian carpet industry, including the companies named in the report, IKEA and Wal-Mart?
What measures will the Commission take to ensure that Indian carpets sold on the European market have been made without resorting to slavery and child labour? Will the Commission urge the Indian Government to take effective action against slavery and child labour in the carpet industry and jointly act against these phenomena? The Commission Staff Working Document on Trade and the Worst Forms of Child Labour of provides a deeper look at the link between international trade and the worst forms of child labour.
The EU strongly supports the ratification and implementation of the fundamental Conventions of the International Labour Organisation ILO , including the abolition of slavery and child labour. Given the existing work, including Commission Documents, the Commission has no plan to carry out a further sector-and country-specific study.
Combating child labour in India has been addressed in the EU-India local Human Rights Dialogue, and EU development cooperation, including through specific projects on child labour. The EU-India dialogue on employment and social policy covers also broader related subjects such as working conditions, social protection. Afgelopen weekend heeft president Museveni aangegeven dat hij de anti-homo wet wil ondertekenen. Indien het geval, hoeveel Europees geld ontvangt Oeganda jaarlijks? Eind januari meldden Belgische media dat een Belgische man in Oeganda was gearresteerd op beschuldiging van homoseksuele relaties.
Deze verbintenissen omvatten onder meer de Universele Verklaring van de rechten van de mens, het Internationaal Verdrag inzake burgerrechten en politieke rechten en het Afrikaanse Handvest van de rechten van de mens en de volkeren. In afwachting van het resultaat van de vergadering zijn alle verdere betalingen voor begrotingssteun bevroren. Last weekend, President Museveni indicated that he was willing to sign it. Is Uganda currently receiving financial assistance from the European Union? If so, how much European funding is Uganda receiving per annum?
At the end of January, the Belgian media reported that a Belgian man had been arrested in Uganda on suspicion of having homosexual relations. Any further budget support payments are on hold until the outcome of their meeting. The existence and activities of foundations operating in the Union for the benefit of the public good are crucial in the fields of education, training, research, historical memory and reconciliation between peoples, protection of the environment, youth and sport, as well as arts and culture, with many of the projects undertaken by such foundations having an impact far beyond national borders.
The foundation, international in its scope and serving also the national community, has as its mission to raise awareness on contemporary art and environmental issues. In view of the various fields of activity of the Serralves Foundation, to which EU funding programmes would it be eligible to apply? When does the Commission expect to have established the legal framework for the European foundation statute? Direct tax issues, including the decision to provide tax incentives for cultural patronage and artistic donations, fall essentially within the competence of Member States.
Hence they are basically free to decide upon their rules in this area, provided that they respect their treaty obligations. A comprehensive European database of cultural projects or institutions does not exist; given the sheer number of institutions across Europe and the diversity of their statutes, it is not clear how practical it would be to create one. The Foundation could potentially apply under the Creative Europe programme, which provides funding to cultural organisations, in particular for cooperation projects, for networks and for platforms.
Grants are awarded following a competitive selection, through calls for proposals. For more information see: Negotiations in the Council are still ongoing. The Commission hopes that Member States will be able to agree on this proposal in the near future. Is the Commission considering adopting legislation to regulate the certification and operation of aircraft with electric motors? If so, what will it contain, what stage are preparations at, and when will it be presented to Parliament?
This regulation does not differentiate the different types of engine. When appropriate safety standards do not exist for the product to be certified, special detailed technical specifications, named special conditions, are prescribed. Currently, there are no specific CS for electrical engines.
There is no need to amend the existing Regulations to take into account the electrical engines. One small electrical engine for powering Powered Sailplans has already been certified in In many EU Member States, married couples enjoy a number of rights and advantages. That often includes tax benefits, together with, for instance, well defined rules on parental responsibility and the possibility of joint health insurance. In many EU Member States, two people of the same sex who marry each other or enter into a registered partnership enjoy the same advantages and rights as a heterosexual married couple.
In connection with the right to free movement, however, it is major problem that many Member States do not recognise same-sex marriages performed in other Member States. In many instances, non-recognition means a loss of rights for the persons concerned, e.
This should be regarded as a hindrance to exercising the right of free movement because, if rights are lost, workers may be stopped from seeking or taking up employment in other EU countries. Accordingly, what will the Commission do to counter the fact that many Member States do not recognise same-sex marriages performed in other Member States. In addition, is the loss of rights to which many of the individuals referred to above are subject, if they are workers moving between Member States in order to seek and take up employment, contrary to the right of free movement?
The Commission is committed to ensure LGBT persons and their family can fully exercise rights to free movement and residence. The Commission has actively intervened when a Member State refused to issue civil status documents for the purpose of entering into a same sex partnership in another Member State and has launched infringement proceedings on the grounds of a Member State's failure to implement the right of same-sex partners to join and reside together with EU citizens there.
For seven years, representative organisations and workers resident on the island, with the consistent support of the Greek Communist Party, have been demanding that the Sea Diamond be raised and that the sea area of the caldera be cleaned from pollution emanating from the wreck.
How does the Commission view this proposal? The Commission wishes to refer the Honourable Member to its replies to earlier questions on this accident, namely: With reference to the points already made in these replies, the Commission would like to reiterate the following four:. This insurance obligation specifically covers, among other maritime claims, the cost of removal and rendering harmless of a shipwreck or any parts thereof.
The Commission continuously promotes the ratification of international maritime conventions, including the Nairobi International Convention on the Removal of Wrecks of Wann rechnet die Kommission mit der Vorlage des genannten Berichts? Die Kommission soll bis September ein strategisches Konzept gegen die Wasserverschmutzung durch pharmazeutische Stoffe entwickeln und bis zum According to a recent report published by Health Care Without Harm Europe, systems are implemented in the majority of Member States, but the level of organisation and implementation is highly variable, and detailed information on their efficiency is scattered and lacking.
Moreover, for some Members States like Bulgaria, Cyprus and Malta there is no indication that such a system is being implemented. The harmonisation of European collection schemes could increase their efficiency, allow comparability among Member States and extend accountability to the pharmaceutical industry and associated players, as well as increase transparency and enforce compliance.
The publication of the report and launch of a public consultation on the issue has been consistently delayed. Does the Commission know if the aforementioned countries, namely Bulgaria, Cyprus and Malta, have implemented a collection scheme for unused pharmaceuticals? If not, what measures is the Commission taking to ensure that these countries fulfil their legal obligations? When does the Commission expect that the aforementioned report will be released?
Will the report and the possible upcoming policy options consider the harmonisation of collection schemes for expired and unused pharmaceuticals at European level? In the development of the strategic approach the Commission will ensure close consultation of all stakeholders as well as the public at large. The Commission has no precise official information regarding the implementation of collection schemes for unused pharmaceuticals by Bulgaria, Cyprus and Malta. The improvement of collection schemes for expired and unused pharmaceuticals by Member States is a policy option likely to be considered in the development of the strategic approach.
How often has the Commission had recourse to the precautionary principal in cases relating to the use of chemicals and other hazardous agents since publication of the aforementioned communication? To date, it has not been necessary to take preventive risk management decisions in accordance with the Precautionary Principle under the REACH restrictions procedure. Opvallend genoeg was gebleken dat de inbreuken zich over meerdere jaren uitstrekten en de periode besloegen van het midden van de jaren negentig tot Waarom heeft de Commissie precies op het moment waarop het Bundeskartellamt een uitspraak heeft gedaan die als uitgangspunt zou kunnen dienen voor een EU-breed onderzoek naar concurrentieverstorende praktijken in de suikersector besloten om haar onderzoek af te breken?
Welke maatregelen is de Commissie van plan op EU-niveau te treffen, gezien het feit dat er nu concreet bewijs voorhanden is van concurrentieverstorende praktijken op de suikermarkten, waar het gevaar van dergelijke praktijken vanwege de hoge mate van concentratie binnen de sector reeds zeer groot was twee derde van alle EU-productierechten is in handen van slechts vier ondernemingen die hun markten zorgvuldig hebben verdeeld? In april hebben ambtenaren van de Commissie onaangekondigde inspecties uitgevoerd in de gebouwen van ondernemingen die actief zijn in de suikerindustrie in verscheidene lidstaten.
De Commissie zocht naar feiten die het bestaan van kartelafspraken tussen leveranciers van witte suiker konden bevestigen. Het onderzoek was niet gericht op de algemene werking van het quotastelsel als dusdanig of op de uitwerkingen ervan op de concurrentie tussen de suikerproducenten.
De Commissie heeft besloten om het onderzoek op dit moment niet verder te zetten. Dit werd vorige maand door onze woordvoerder meegedeeld. Het onderzoek van de Commissie dat inmiddels werd gesloten, betrof mogelijk concurrentieverstorend gedrag in een andere periode dan die welke door het Bundeskartellamt werd onderzocht.
Bovendien zijn ook de activiteiten die het onderwerp vormden van beide onderzoeken niet noodzakelijkerwijs dezelfde. De afsluiting van het onderzoek van de Commissie houdt dan ook geen verband met de conclusies van het onderzoek van het Bundeskartellamt. De Commissie sluit niet uit dat zij de suikersector in een later stadium opnieuw aan een onderzoek zal onderwerpen, op basis van nieuwe elementen afkomstig van nationale mededingingsautoriteiten of andere bronnen.
Sectoren met een sterke concentratie van bedrijven, zoals de suikerindustrie, zijn gevoelig voor kartelvorming zoals opnieuw wordt bevestigd door de conclusies van het onderzoek van het Bundeskartellamt. Deze sectoren verdienen de aandacht van mededingingsautoriteiten in de hele EU, inclusief de Commissie. Dit is precies waarom de Commissie in optrad en niet zal aarzelen om opnieuw op te treden, indien en wanneer dit nodig is. It is striking that the infringements were found to have taken place over several years up to , in some cases dating back to the mids.
Why has the Commission decided to abandon its investigation precisely at a time when the Bundeskartellamt has provided a potential springboard for an EU-wide investigation into anti-competitive behaviour in the sugar sector? The Commission searched for facts that could confirm the existence of cartel agreements between suppliers of white sugar. The investigation did not target the overall functioning of the quota system as such or its effects on competition between sugar producers. As the Commission's initial suspicion as to the existence of collusion between the sugar producers in various EU countries was not conclusively confirmed by the information gathered on the spot, the Commission decided not to pursue this investigation at this point in time.
This was communicated by our spokesperson last month. The investigation of the Commission that has now been closed searched for possible anti-competitive behavior in a time period different from that investigated by the Bundeskartellamt. Nor is the behaviour targeted by both investigations necessarily the same. The closure of the Commission investigation has therefore no relation with the conclusions of the Bundeskartellamt investigation. The Commission does not exclude that it may re-investigate the sugar sector at a later stage, on the basis of new elements originating from national competition authorities or otherwise.
Highly concentrated sectors, such as the sugar industry, are sensitive to cartel behaviour, as again confirmed by the conclusions of the investigation of the Bundeskartellamt. This is exactly why the Commission acted in , and the Commission will not refrain from doing this again, if and when necessary. Can the Commission state what action it has or will be taking in its role of supporting Member States in the implementation of welfare reforms to ensure that EU citizens are not discriminated?
Social policy is primarily a matter of national competence. However, the Commission provides the Member States with support to promote social inclusion, including in the areas of housing exclusion and homelessness. Through the European Semester process, the Commission sets overall budget, economic and social priorities, and gives policy guidance to boost growth, employment and social cohesion in line with the EU's long-term growth strategy.
The Semester process allows practical recommendations to be issued in the social field. Under the social open method of coordination, the Commission supports the Social Protection Committee in mobilising various instruments to tackle poverty and social exclusion. The direct aids envelopes for EU and EU-2 were established on the basis of the same unit values as for the EU, using the actual yields, tonnes and numbers of animals, and resulting from the accession negotiations.
Irrespective of the allocations, direct aids in the Member States that joined the European Union after are subject to the principle of gradual introduction phasing-in. Since their accession, the payments to these Member States have constantly increased as a result of the phasing-in. For information and as regards rural development, Member States must adopt multiannual programmes which are always progressively implemented over the programming period.
As a result, payments are usually very low the first year of programming irrespective of the amounts commitment appropriations allocated to programmes. The UK Government has submitted an application to the Commission for 17 of the most rural areas in mainland UK to receive a fuel duty discount of up to five pence per litre. Can the Commission provide an updated timescale for the implementation of this rebate? How many road users does the Commission estimate could benefit from this rebate, should it be approved? Depending on this assessment the Commission will decide whether to make a proposal for a Council Decision.
At this early stage it is difficult to provide an exact timetable for a possible implementation of this measure. The Commission cannot comment at this stage on this question but would encourage the Honourable Member to contact the UK authorities about their estimate in this regard. Could the Commission detail the action taken to address these concerns since the adoption of the aforementioned resolution?
In its contacts with the Chinese authorities, the EEAS has regularly raised concerns about the re-education through labour system, the death Penalty and Freedom of Religion or Belief, with particular reference to Falun Gong followers. Can the Commission provide an update on the current state of negotiations with the Faroe Islands and Iceland? Is the Commission considering further punitive measures against the Faroe Islands and Iceland? What is the latest scientific advice the Commission has received on mackerel stocks, and how will this influence the ongoing negotiations with the Faroe Islands and Iceland?
While Iceland does not yet adhere to this arrangement, provisions have been made for this country to join and adopt a total allowable catch in coherence with the catch limitations adopted by the other parties. The exchanges with Faroe Islands were particularly welcomed by the fishing industries of both parties given that since there had been no agreement on them. The latest scientific advice available from ICES recommends total catches at around t.
The TAC agreed by EU, Faroe Islands and Norway is somewhat higher for the first year, but the Commission does not believe this level puts the stock in jeopardy, as ICES also notes that the size of the stock is much higher than previously thought. Norway is the EU's main partner in the management and exploitation of the mackerel stock and is therefore an important partner in the consultations.
In its recent White Paper on a possible independent Scotland, the Scottish Government made a series of assertions relating to how it could maintain certain advantages relating to its current UK and EU membership. Specifically relating to the charging of university tuition fees, it stated: The Commission recalls that non-compliance by a MS with Union law provisions constitutes a failure by that MS to fulfil its obligations under the Treaties. The Maltese Government is to establish a small tourism police unit that will have roughly 25 uniformed officers based in places related to tourism.
Is the Commission aware of any similar system adopted by any of the other Member States? In addition, EU Member States regularly second police officers to other EU Member States to assist local police officers in cases where large numbers of tourists are expected in the host country. This has for example been done in France and Croatia. X'diffikultajiet huma mistennija f'dan ix-xenarju? The Commission has expressed its regret over the result of the Swiss referendum on the initiative for the introduction of quantitative limits to immigration.
Such an initiative runs counter to the established freedom of movement of people between the European Union and Switzerland. How does the Commission intend to address this situation? What difficulties are envisaged within this scenario? How will the referendum result affect the obligations which must be fulfilled by Switzerland within the European internal market? The referendum introduced a new article into the Swiss constitution which only takes effect once the necessary implementing legislation is adopted. Compliance of the implementing legislation with the EU-Swiss Agreement on the free movement of persons as well as any possible initiatives will be analysed once the details of the draft legislation are known.
At the same time, action by the Commission will be considered. The Swiss government has assured the European Union following the referendum that it will continue to honour its existing international obligations, including those within the internal market. The European Commission, for its part, also considers that pacta sunt servanda and will continue to fulfil its obligations under the bilateral agreements. It has been reported that the possibility of introducing home schooling is being considered.
The Commission does not dispose of any systematic information on the issue of home schooling provisions in the Member States. This includes all possible forms of provisions including, if relevant, special forms, such as home schooling. The Commission has issued a communication containing a number of concrete actions to reform the way in which the Internet is managed and run.
The communication calls for more transparent, accountable and inclusive Internet governance. The Commission has invited the Council, Parliament, the Economic and Social Committee, the Committee of the Regions and the Member States to agree on a common vision, such as that highlighted in the communication, and to defend it jointly in upcoming international debates. To this end, does the Commission plan on opening negotiations with non-EU countries on this matter in order to hold an even stronger position during upcoming international debates?
The European Commission has engaged with a number of third countries and stakeholders organisations on matters related to the global governance of the Internet for some years. The recently adopted Communication on Internet Policy and Governance confirms the line taken so far, including on the basis of positions adopted by the European Parliament, in particular for what concerns the need to safeguard and strengthen the multi-stakeholder model and to make sure the governance framework and core Internet functions are truly globalised.
For the time being, the European Commission does not envisage proposing the opening of any formal negotiation with third countries on these matters. The communication on Internet Policy and Governance does not call for any new international legal instrument to address the issues of Internet governance. Can the Commission provide any information about whether the objectives of the Centre have been fulfilled in terms of protecting European citizens and businesses against online threats and challenges? How is the European Cybercrime Centre cooperating with Member States to address these challenges and raise awareness among online users?
The European Cybercrime Centre within Europol EC 3 has had a successful first year of existence, assisting in the coordination of 19 major cybercrime operations in its areas of focus, which are cyber attacks, child sexual abuse and non-cash payment fraud.
Internal medicine
The EC 3 works closely with Member States on these and other on-going operations. Structural cooperation also takes place in the context of the EMPACT Policy Cycle , for which cybercrime cyber attacks, child sexual abuse and non-cash payment fraud is one of the priorities. The EC 3 is a co-driver for each of the three cybercrime areas mentioned. Representatives of participating Member States and the EC 3 meet at least four times a year to coordinate activities. In terms of raising awareness, EC 3 cooperates closely with actors across communities, including the private sector and other EU agencies, and regularly provides analysis and explanations of current threats and trends to its stakeholders.
Future plans for awareness-raising also include participating in the European Cybersecurity Month and other events. How does the Commission monitor, if at all, the transition of students suffering with dyslexia and specific learning difficulties from education into the work force in different Member States? The Agency provides analysis, evidence and information about inclusive education across Europe; it issues policy recommendations and provides tools to monitor progress.
Linee-guida e Raccomandazioni
The project analysed the extent to which VET programmes for learners with special needs which includes people with dyslexia prepare them to succeed in the labour market. What support is provided to students in higher education suffering from dyslexia and specific learning difficulties? Student support is the responsibility of national authorities and there is a diversity of national support measures for dyslexic students, ranging from extra IT support, scanning of textbooks into audio files, more time to complete written exams or extra grants.
The European Union, in its role of supporting Member States, is also active in this area. The Commission supports the European Agency for Special Needs, which facilitates the collection, processing and transfer of European level and country-specific information to its Member States enabling them to learn from each other through exchange of experience and best practice.
The Commission also supports the Member States through evidence-based policy making to address common challenges. How does the Commission envisage Internet governance as part of the European standards of human rights and fundamental freedoms? Can the Commission provide information as to whether Internet governance may lead to conflicts with other established human rights and fundamental freedoms?
What steps does the Commission plan to take to assess whether the training and support it has provided for teachers and other professionals within the education sector to ensure that dyslexic pupils are identified earlier, and receive quicker access to the support they need, is meeting the stated objectives? What steps is the Commission taking to ensure that teachers have the knowledge and skills to be able to identify those children who are at risk of specific learning difficulties such as dyslexia?
How is the Commission monitoring the level of awareness and expertise on dyslexia and specific learning difficulties among school staff in different Member States? Member States are responsible for the organisation and content of their education systems, including the training and support for teachers. The Commission supports collaborative work, exchange of good practice, and peer learning between MS in order to find solutions to common challenges. The Commission established a High Level Group of experts in the field of Literacy to examine research, effective policies, and good practices to reduce the number of people who lack basic reading and writing skills.
They concluded that struggling readers primarily need specific educational support dedicating adequate time and applying the proper method to support them to acquire reading skills. They also found that programmes aimed at improving the skills of struggling readers have a high rate of success and are extremely cost-effective.
What proportion of qualified teachers in Member States received dyslexia-SpLD awareness training as part of their continuing professional development in the latest period for which figures are available? There is no EU-level data available regarding the proportion of qualified teachers that received dyslexia-SpLD training. Although these data do not specifically cover continuing professional development on Dyslexia and SpLD, the report highlights how future teachers are prepared to tackle reading difficulties.
Knowledge and skills for teaching reading in initial teacher education: In EU health ministers unanimously adopted a Council recommendation on cancer screening setting out best-practice principles for early detection of cancer and inviting all Member States to implement national, population-based screening programmes for breast, cervical and colorectal cancer.
According to the National Cancer Plan , a colorectal cancer screening programme is currently being introduced. According to the information available to the Commission, a national programme for cervical cancer screening has not been introduced so far. Their employers would get a percentage of the social benefits paid to the workers for three years. Is the Commission aware of any similar social benefits in the other Member States?
Earning disregards do exist in most Member States, although they vary in level and duration. For unemployment benefits there is a section dedicated to the accumulation with earnings from work and similar information are reported for other benefits. In addition, on taking up employment, employers can be given incentives.
According to an air quality study carried out by an independent body, the levels of minute airborne pollutants recorded near the heavy fuel oil plant in Delimara fall within EU limits. Following this assessment, can the Commission provide information on whether the Delimara power station conforms with EU legislation on air quality? The Commission does not collect monitoring data concerning emissions of individual power plants or other industrial installations.
It is up to the competent national authorities to ensure that the permit conditions and emission limit values are complied with. Recent cases of animal cruelty in Malta have raised a debate as to whether new legislation with more effective deterrents should be introduced to fight animal cruelty. Is the Commission aware of the enforcement systems adopted by any of the other Member States as deterrents to fight animal cruelty?
The Commission in adopted an Animal Welfare Strategy which set out a number of actions for which it has competence and already performed such as: It also set out a number of actions which it proposed to consider during the period covered by the strategy However the Commission, does not request information on the means and method of enforcement of laws prohibiting animal cruelty in general in the Member States which remains the competence of the Member States. Could the Commission provide an estimate of the total savings for EU consumers from the reduction in roaming costs since ?
Could the Commission clarify whether the roaming legislation, restricting the price of calls, texts and data, would apply to a UK phone number calling an Irish phone number while on holiday in Spain? Yes, current EU roaming legislation applies, and the roaming provisions in the Connected Continent proposal would apply, to a UK phone number calling an Irish phone number while on holiday in Spain. In order to achieve significant advancement in the lives of disabled people and their families, to safeguard their social inclusion, and to ensure that the relevant and necessary legislative measures are taken, we consider the establishment of a European Commission directorate, and not simply a unit within one, which is specifically responsible for disability affairs to be of paramount importance.
Therefore, we, as responsible MEPs, would like to know ask the following questions:. Has the Commission has ever considered establishing a directorate responsible exclusively for disability affairs? This ensures that the needs and rights of people with disabilities are taken into consideration when relevant new legislative proposals and initiatives are prepared and also in the implementation of EU policies and actions.
Compliance of new proposals with the CRPD is checked systematically following the operational guidance on taking account of fundamental rights in Commission impact assessments. Kann die Kommission angeben, ob die Studie gegebenenfalls folgende Aspekte umfassen wird. Zugang zu Medikamenten zur Behandlung von Multiple Sklerose. Wenn ja, wann kann sie damit beginnen? Can the Commission state whether, when it launches such a study, it will focus on the following aspects:.
If so, when will it be ready to begin? If not, can it give specific reasons for its unwillingness? Against this background, and also given the existence of the study referred to and of further reports on this subject, the Commission has no plans to launch itself a similar study on access of people with multiple sclerosis to healthcare in EU-Member States. EU research funding is granted on the basis of competitive calls for proposals, following an independent peer-review evaluation.
Could the Commission please provide detailed examples and a list of the Member States concerned. Those patients who choose to use these rights may do so on the grounds that going to another Member State for healthcare may help them access better, more specialised or swifter care — which may make a considerable difference to their lives. National contact points which Member States are required to establish under this directive provide a certain amount of information to ensure that patients are in a position to actually use these rights e.
This increase in transparency will benefit all patients, not only those who choose to travel abroad. The Commission is not in a position to know how many patients have used this directive or for which treatments. The firing of rubber bullets by agents of the Spanish Guardia Civil force against hundreds of immigrants who were trying to enter Spain by crossing the border at Ceuta represents a summary expulsion en masse that contravenes European and local laws on immigration.
Both sets of laws prioritise the duty of succour over any other consideration and establish that, before any expulsion process is initiated, assistance must be provided to the people affected, each case must be treated individually, checks must be made to see whether any conditions apply that would allow them to enter the country legally, and at any event expulsion orders must be individualised.
This incident, which to date has led to the deaths of fifteen people, stands in contrast to the manner in which this semi-military force has acted on previous occasions. Up until now, they had not used these means to deal with the problem of illegal immigration but instead had responded with rescue and assistance operations for people found in difficulties in small boats at sea. In this case, in view of the breach of fundamental principles such as those referred to above:. What specific explanations has the Commissioner requested from the Spanish authorities?
Does the Commission intend to ask for these recordings from the Spanish authorities? She welcomed the initiative of the Spanish authorities to carry out a full inquiry into the incident and considered that the inquiry should look into the use of force and the alleged summary return of migrants to Morocco. It is not Commission policy to comment on unofficial versions of events. The Commission will wait for the outcome of the inquiry being carried out by the Spanish authorities.
The Commission considers that the steps identified by the Task Force Mediterranean in the aftermath of the Lampedusa tragedies will allow Member States to better manage irregular migration at their borders. Work on the implementation of these actions is in progress. Det danske program ligner til forveksling det svenske og finske program. Since , Denmark has had a coherent Salmonella programme which ensures full traceability of more types of Salmonella than are required under the regulation.
Adding liraglutide to lifestyle changes, metformin and testosterone therapy boosts erectile function in diabetic obese men with overt hypogonadism. Peripheral neuropathy and the risk of cardiovascular events in type 2 diabetes mellitus. Patient education for preventing diabetic foot ulceration. Per la diagnostica della neuropatia autonomica CV sono necessari sempre 3 test: Alcuni esami diagnostici e terapie riportati in tab.
Come gestire la malattia cardiovascolare nei diabetici? Gli obiettivi per la riduzione del rischio CV sono sintetizzati nella tabella 7. Hypoglycemia from a cardiologist's perspective. Clin Cardiol , Cardiovascular Disease and Risk Management. Importante anche il monitoraggio annuale con ECG alla ricerca di anomalie della ripolarizzazione, sovra-slivellamenti, extra-sistolia sopra-ventricolare, ecc e bi-triennale con ecocardiografia per ricercare segni precoci di cardiopatia metabolica, quali disfunzione diastolica, alterazioni della funzione ventricolare, discinesie, ecc che possono preludere a un evento ischemico acuto ADA.
Cardiovascular disease and risk management. Quando le modificazioni dello stile di vita non ottengono un decremento ponderale adeguato, deve essere preso in considerazione il ricorso alla terapia farmacologica Grado A; MLE 1. I pazienti con DM2 che vengono sottoposti a procedure che inducono malassorbimento come il by-pass gastrico Roux-en-Y o la diversione bilio-pancreatica con switch duodenale devono seguire un attento follow-up post-operatorio, a causa del rischio di ipoglicemia e di deficit di micro-nutrienti Grado D; MLE 4.
Questi farmaci migliorano i valori pressori e lipidici, prevengono la progressione a DM e migliorano il controllo glicemico e lipidico nei pazienti con DM2. La chirurgia bariatrica deve essere presa in considerazione solo dopo fallimento delle terapie comportamentali e farmacologiche.
Inverse relationship between body mass index and mortality in older nursing home residents: Obes Rev , Surgical versus medical treatment of type 2 diabetes mellitus in nonseverely obese patients: Ann Surg , Laparoscopic Roux-en-Y gastric bypass versus sleeve gastrectomy for obese patients with type 2 diabetes: Am Surg , Douglas IJ, et al. Bariatric surgery in the United Kingdom: PLOS Med , Questa condizione deve essere sospettata sulla base di una storia di sonnolenza diurna e di russamento, soprattutto se un familiare conferma fasi di apnea.
La valutazione da parte di uno specialista del sonno deve essere considerata nel sospetto di OSA o di sindrome delle gambe senza riposo e quando i pazienti sono intolleranti agli apparecchi a pressione positiva continua CPAP Grado A; MLE 1. Obstructive sleep apnea as a risk factor for type 2 diabetes mellitus. Nat Sci Sleep , 7: Nei pazienti non critici la gestione della glicemia deve essere effettuata secondo schemi di somministrazione sottocutanea, che comprendano una quota basale e somministrazioni per gli apporti nutrizionali e le eventuali correzioni glicemiche Grado A; MLE 1.
La somministrazione deve essere sincronizzata con i pasti, la nutrizione enterale o quella parenterale Grado A; MLE 1. In tutti i pazienti ospedalizzati, indipendentemente da una precedente diagnosi di DM, deve essere misurata la glicemia Grado C; MLE 3. In tutti i pazienti con DM noto e nei non diabetici sottoposti a terapie a rischio di provocare iperglicemia, come i corticosteroidi e la nutrizione enterale o parenterale, deve essere intrapreso il monitoraggio del glucosio con determinazione al letto del paziente POC Grado D; MLE 4.
I pazienti con iperglicemia persistente richiedono un protratto monitoraggio POC con trattamento analogo a quelli con storia nota di DM. La gestione domiciliare del DM deve iniziare immediatamente dopo la dimissione e a questo scopo devono essere fornite al paziente delle chiare istruzioni che lo guidino Grado D; MLE 4.
Intense metabolic control by means of insulin in patients with diabetes mellitus and acute myocardial infarction DIGAMI 2: Eur Heart J , Fullerton B, et al. Intensive glucose control versus conventional glucose control for type 1 diabetes mellitus. Cochrane Database Syst Rev , 2: Le iniezioni multiple, tuttavia, possono costituire un problema in alcuni contesti scolastici. Nei bambini e negli adolescenti con DM2, devono essere dapprima impiegate le modificazioni della dieta e dello stile di vita Grado A; MLE 1.
Gli adolescenti con DM1 devono essere trattati in stretta collaborazione con il paziente e i suoi familiari. Tutte le donne con DM in atto DM1, DM2 o pregresso GDM devono avere accesso alle cure prima del concepimento, in modo da assicurare un apporto nutrizionale adeguato e il controllo metabolico al momento del concepimento, durante la gravidanza e nel post-partum Grado B; MLE 2. Come basale suggeriamo di evitare NPH e detemir rischio di ipoglicemie e preferire glargine. Il SMBG deve essere effettuato in tutti i pazienti in terapia insulinica, con un minimo di due determinazioni giornaliere e — idealmente - prima di ogni iniezione di insulina Grado B; MLE 2.
Anche i pazienti che non richiedono la terapia insulinica traggono vantaggio dal SMBG, soprattutto per il feed-back fornito sugli effetti del loro intervento farmacologico e sullo stile di vita. La frequenza dei controlli deve essere personalizzata. Continuous glucose monitoring systems for type 1 diabetes mellitus.
Cochrane Database Syst Rev , 1: Poolsup N, et al.
Systematic review and meta-analysis of the effectiveness of continuous glucose monitoring CGM on glucose control in diabetes. Diabetol Metab Syndr , 5: Revisione sistematica e valutazione economica su 74 studi. Regno Unito; prospettiva amministrativa del sistema sanitario nazionale. Meta-analisi del trattamento con CSII da oltre 50 studi. CSII ha portato a miglioramento dei risultati clinici a lungo termine per il miglior controllo glicemico rispetto a MDI.
Il team deve comprendere medico di medicina generale, endocrinologo, infermiere con competenza specialistica, dietista, fisioterapista e psicologo. La gestione terapeutica dello stile di vita deve essere valutata e discussa con tutti i pazienti con DM o Prediabete, sia al momento della diagnosi che nel corso della vita successiva Grado D; MLE 4. Quali vaccinazioni dovrebbero essere fatte nei diabetici? I pazienti con DM possono necessitare di ulteriori vaccinazioni per proteggersi nei confronti di altre malattie infettive. La vaccinazione anti-influenzale viene effettuata in Italia ai pazienti particolarmente fragili quali i diabetici.
Vaccines for the prevention of seasonal influenza in patients with diabetes: BMC Med , I pazienti affetti da depressione dovrebbero essere presi in carico dagli specialisti in psicologia che fanno parte del team per la cura del DM Grado D; MLE 4. Anche se esiste una relazione tra s. The association between diabetes and depression: Glucose metabolism and antidepressant medication. Curr Pharm Des , Inoltre, questi pazienti devono essere sottoposti con maggiore frequenza e attenzione rispetto alla popolazione generale allo screening delle neoplasie associate con i disordini metabolici Grado B; MLE 2.
Il team diabetologico dovrebbe essere attento alle possibili associazioni e raccomandare interventi terapeutici basati sul profilo di rischio individuale del paziente Grado D; MLE 4. Grado D; MLE 4. Il diabete correla con aumentato rischio di cancro del pancreas Wang M, et al. Cancer risk among patients with type 2 diabetes mellitus: Sci Rep , 5: Effect of metformin on cancer risk and treatment outcome of prostate cancer: PLOS One , 9: Zhang ZY, et al. Reduced risk of lung cancer with metformin therapy in diabetic patients: Am J Epidemiol , The prognostic value of metformin for cancer patients with concurrent diabetes: Diabetes Obes Metabol , I conducenti di veicoli commerciali sono ad alto rischio di sviluppare DM2.
Le persone affette da DM che sono impegnate in specifiche occupazioni, come i conducenti, i piloti, gli anestesisti e coloro che effettuano immersioni, richiedono specifiche attenzioni gestionali, focalizzate in primo luogo su trattamenti che riducano il rischio di ipoglicemia Grado C; MLE 3. The majority of recommendations are EL 1 or 2: The evidence base presented here provides relevant information for the recommendations in the Executive Summary. Come indagare e diagnosticare il Diabete Mellito? DM refers to a group of metabolic disorders that result in hyperglycemia, regardless of the underlying etiology.
DM is diagnosed by using any of 3 established criteria for elevated blood glucose concentrations Table 6 17 [EL 4; consensus NE]. Moreover, A1C is known to be affected by nonglycemic factors such as changes in red blood cell maturity and survival and impaired renal function, and it may be unreliable as a measure of glycemic burden in some patients from certain ethnic groups, including those of African American and Latino heritage 20 [EL 3; SS]; 21 [EL 4; review NE]; 22 [EL 3; SS]. On the basis of these limitations, A1C measurement cannot be recommended as a primary method for diagnosingDM.
The diagnosis of DM is best confirmed by 1 of the 3 established direct measures of plasma glucose, with A1C as a secondary criterion Table 6. In the absence of unequivocal hyperglycemia, the same type of test should be repeated on a different day to confirm the diagnosis of DM because of glucose level variability 23 [EL 4; review NE]. DM is classified into T1D, T2D, GDM, monogenic DM, and other less common conditions such as chronic pancreatitis, pancreatic resection, or rare insulin resistance and mitochondrial syndromes.
In a minority of patients with T1D, evidence for autoimmunity is lacking, and the etiology of islet destruction is unclear. Prevention of T2D depends upon systematic lifestyle modifications including caloric intake reduction e. Weight-loss surgery may normalize glycemia in patients with prediabetes, prevent the appearance of overt T2D, and reduce its progression.
For patients in whom lifestyle modification after 3 to 6 months has failed to produce necessary improvement, pharmacologic intervention may be appropriate. In fact many, if not the majority, of patients will benefit from starting medications concomitantly with lifestyle intervention, just as in other metabolic diseases.
More extensive discussion can be found in the American College of Endocrinology consensus on the management of prediabetes 31 [EL 4; consensus NE]. One of these studies reported a reduction from Orlistat therapy is also associated with decreases in A1C; in 1 study, A1C decreased by 1.
These reductions were related to the degree of weight loss A large-scale study specifically examining the effect of liraglutide on the incidence of T2D is underway. There is no dispute that elevated glucose levels are associated with micro- and macrovascular complications of DM. What have remained under debate are the specific targets for glucose control in patients with DM. However, it is unknown whether treating patients with DM—some with pre-existing diabetic complications—using complicated regimens to force glucose concentrations into the normal range actually prevents or delays those complications.
How is hypoglycemia managed? No RCTs have yet established optimal glycemic targets. Professional organizations have relied on results from existing intervention trials achieving improved A1C levels and epidemiologic analyses of various studies to arrive at consensus statements or expert opinions regarding targets. In all cases, the potential risks of intensive glycemic control may outweigh its benefits, especially in patients with frequent severe hypoglycemia, hypoglycemia unawareness, or a very long duration of DM, particularly in the presence of established and advanced atherosclerosis, advanced age, and terminal illness.
How are glycemic targets achieved? The components of therapeutic lifestyle changes include healthful eating, regular physical activity, sufficient sleep, avoidance of tobacco products, limited alcohol consumption, and stress reduction. Nutritional medicine in DM comprehensive care consists of 3 components: The last category applies to those patients receiving enteral or parenteral nutrition in which medications provided for glycemic control must be synchronized with carbohydrate delivery; however, this topic is beyond the scope of this CPG.
The physician or a registered dietitian should discuss these recommendations in plain language with patients at the initial visit after DM diagnosis and then periodically during follow-up office visits 4 [EL 4; NE]. Comments should be broad and nontechnical, about foods suitable for the general population including those without DM that promote health versus foods that may promote disease or disease complications. Discussions between patients and healthcare professionals should include information on specific foods and meal planning, grocery shopping, and dining-out strategies. MNT addresses the metabolic needs of patients with DM and involves a more detailed discussion, usually in terms of calories, grams, and other metrics.
The goal is to intensify efforts of healthy eating behaviors aimed at optimizing glycemic control and reducing the risks of DM complications. These recommendations should also be discussed and implemented by the physician or a registered dietitian for all patients with DM. All patients should be advised how to achieve and maintain a healthful weight. For overweight individuals with a BMI of 25 to In a randomized comparison of the Atkins, Ornish, Weight Watchers, and Zone diets, weight change did not differ between diets about 5 kg , and adherence to the diet was the single most important criterion of successful weight loss 90 [EL 1; RCT, single blinded].
Patients unable to accomplish this should be referred to a registered dietitian or weight-loss program with a proven success rate. In areas underserved by registered dietitians, physicians should take on more responsibility during patient encounters for nutritional counseling and reinforcing healthful eating patterns.
Key recommendations address the need for consistency in day-to-day carbohydrate intake, adjusting insulin doses to match carbohydrate intake e. The magnitude of weight loss after 1 year in Look AHEAD was related to the frequency of using meal replacements, amount of physical activity performed, and attendance at behavioral sessions 96 [EL 1; RCT]. Because physical activity is usually combined with caloric restriction and weight loss, as in combined lifestyle intervention programs, distinguishing the effects of increased physical activity alone from those of calorie restriction and weight loss is often difficult.
Regular physical exercise—both aerobic exercise and strength training—is important to improve a variety of CVD risk factors, decrease the risk of falls and fractures, and improve functional capacity and sense of well-being [EL 4; commentary NE]. Physical activity is also a main component in weight loss and maintenance programs. Activity of at least minutes per week of moderate-intensity exercise such as brisk walking e. For persons with T2D, recommendations include flexibility and strength training exercises in addition to aerobic exercise [EL 1; RCT].
The 1-year results revealed a significant association between minutes of physical activity and weight loss, indicating that those who were more active lost more weight 96 [EL 1; RCT]. The benefits and risks of increasing physical activity and the practical aspects of implementing a physical training program in people with T2D are discussed in detail in a position paper [EL 4; consensus NE]. People with T1D generally experience the same benefits of regular physical exercise as T2D patients.
However, patients requiring insulin therapy must also learn about the acute and chronic effects of exercise on glucose regulation and how to adjust insulin dosages and food intake to maintain glucose control before, during, and after exercise to avoid significant hypoglycemia or hyperglycemia [EL 4; NE].
The final component of therapeutic lifestyle change is the use of behavior modification strategies in support of healthy eating and regular activity. However, several studies have shown that attempts to include lifestyle change counseling as part of routine primary care fail to help patients achieve or sustain weight loss. In addition, the initial success of a structured lifestyle program may fade without continued support [EL 1; RCT, not blinded] , suggesting that ongoing behavioral strategies in addition to education on healthy eating and physical activity should be included in lifestyle intervention programs.
The results demonstrated that extended behavioral support within an intensive lifestyle intervention program helps facilitate meaningful weight loss for up to 8 years 95 [EL 1; RCT, not blinded]. The goal of glycemic treatment in subjects with T2D is to achieve clinical and biochemical targets with as few adverse consequences as possible. As monotherapy, most oral antihyperglycemic agents reduce A1C by 0. Larger decrements are seen in patients with more marked A1C elevations, likely explaining the apparent greater efficacy of older agents versus newer ones 4 [EL 4; NE].
However, the various classes of glucose-lowering agents differ widely in other respects Table 9.
Buy Il diabetico anziano. Gestione condivisa (Italian Edition): Read Kindle Store Reviews - www.farmersmarketmusic.com Il diabetico anziano. Gestione condivisa (Italian Edition) eBook: Claudio Marengo , Marco Comoglio, Andrea Pizzini: www.farmersmarketmusic.com: Kindle Store.
In addition to lowering glucose, the priority in DM management is to minimize the risks of hypoglycemia and weight gain. Metformin may have anorectic effects, is sometimes associated with weight loss, may cause gastrointestinal GI adverse effects e. Metformin should be continued as background therapy and used in combination with other agents, including insulin, in patients who do not reach their glycemic target on monotherapy.
TZDs, sulfonylureas, and glinides may also be used, although caution should be exercised owing to the potential for weight gain, hypoglycemia, or other risks. Sulfonylureas and glinides increase insulin secretion in a glucose level-independent fashion. For unknown reasons, not all patients with T2D respond to sulfonylureas primary failure , and antihyperglycemic effectiveness declines after several years of treatment in many patients secondary failure [EL 1; RCT].
The main side effect of the sulfonylureas is hypoglycemia, which can be more prolonged than that produced by insulin, particularly when longer-acting formulations are used in the elderly [EL 4; NE]. Renal insufficiency also increases the risk of sulfonylurea-associated hypoglycemia.
Clinical studies and meta-analyses of RCTs reported that treatment with pioglitazone results in a statistically significant reduction in the composite outcome of nonfatal acute myocardial infarction, stroke, and all-cause mortality [EL 1; MRCT]. TZDs may also cause fluid retention particularly in patients with cardiac or renal disease , which may contribute to TZD-associated weight gain and peripheral edema.
According to the FDA, pioglitazone, but not rosiglitazone, may be associated with increased rates of bladder cancer, although there is not enough evidence to support a clear association [EL 4; NE]. A recent cumulative exposure analysis involving data from 1. In addition to glucose lowering, the GLP-1 receptor agonists may slow gastric emptying, promote early satiety, and reduce food intake, which may result in weight loss. Currently approved GLP-1 receptor agonists include albiglutide, dulaglutide, exenatide, and liraglutide, which are administered by injection on a twice daily, daily, or weekly basis.
All of the studies show equivalent or slightly better A1C lowering by GLP-1 receptor agonists with the advantages of a 2- to 3-kg weight loss and little or no additional hypoglycemia. In rodents, GLP-1 receptor agonists may increase the frequency of benign and malignant C-cell neoplasms; however, in humans, neither acute pancreatitis nor medullary thyroid carcinoma has been convincingly shown to be caused by incretin-based therapies [EL 4; NE]. Nevertheless, GLP-1 receptor agonists should be used cautiously in patients with a history of pancreatitis and discontinued if acute pancreatitis develops during use.
All GLP-1 receptor agonists except twice-daily exenatide are contraindicated in patients with a personal or family history of medullary thyroid carcinoma and in patients with multiple endocrine neoplasia syndrome type 2. The FDA has stated that patients taking a GLP-1 receptor agonist do not need to be monitored for medullary thyroid carcinoma e. DPP-4 inhibitors do not cause weight gain; they can be administered in patients with CKD at full dosage when not cleared by the kidneys linagliptin or with appropriate dose adjustment for agents that are renally cleared sitagliptin, saxagliptin, alogliptin ; they lack significant GI adverse effects [EL 4; opinion NE] ; and they have been associated with reduction in cardiovascular events in analyses of registration trials [EL 1; MRCT] , although neither benefit nor harm was seen in cardiovascular outcome studies conducted in subjects with advanced CVD in placebo-controlled, randomized studies with alogliptin or saxagliptin [EL 1; RCT]; [EL 1; RCT].
The trial comparing saxagliptin with placebo showed an increased likelihood of hospitalization for congestive heart failure and an increase in hypoglycemia [EL 1; RCT] ; this should lead to caution in the use of this agent in persons with a history of heart failure who also have existing CVD. The main adverse effects noted with DPP-4 inhibitors are a small increase in upper respiratory tract viral infections rates of nasopharyngitis were 6. The glucosuric effect of these agents leads to weight loss in most patients. Most patients also experience decreases in systolic blood pressure.
Elderly patients on loop diuretics need to be monitored for postural hypotension. Because they exert their glycemic effects in the kidney, these agents have limited efficacy in patients with CKD. Also, by increasing glycosuria, SGLT2 inhibitors may increase the risk of urinary infection and fungal genital tract infection. Dehydration due to increased diuresis could lead to hypotension and adverse cardiovascular effects, although no cardiac safety signals have been reported [EL 4; NE].
Bone fracture has been described in postmarketing safety reporting. As with all new agents, aggressive postmarketing surveillance for SGLT2 inhibitor adverse effects is ongoing. Colesevelam carries a low risk of hypoglycemia and also reduces LDL-C, for which it was originally developed. Its main adverse effect is constipation, but it is not systemically absorbed and therefore is not likely to have systemic adverse effects [EL 4; NE]. The dopamine receptor agonist bromocriptine does not cause hypoglycemia. It can cause nausea and orthostasis and should not be used in patients taking antipsychotic drugs.
Because many patients do not achieve adequate glycemic control with monotherapy, combining antihyperglycemic agents is often appropriate 4 [EL 4; NE]. Sulfonylureas, in contrast, are problematic when used in combinations because they can cause hypoglycemia and may reduce, eliminate, or minimize the weight-loss benefit of drugs such as metformin, GLP-1 receptor agonists, and SGLT2 inhibitors [EL 2; MNRCT].
The traditional postponement of insulin therapy after prolonged failure of lifestyle and oral agents to achieve glycemic control has been revised in the last decade to incorporate primarily basal insulin therapy much sooner, often in combination with oral agents or GLP-1 receptor agonists 4 [EL 4; NE]; [EL 4; NE]. Insulin therapy may be initiated as a basal, basal-bolus, prandial, or premixed regimen, although for most patients, starting with a basal insulin analog added to the existing antihyperglycemic regimen is preferred Table 11 4 [EL 4; NE].
The combination of insulin with any antihyperglycemic agent raises the potential for hypoglycemia. Patients should be closely monitored, and those on sulfonylureas or glinides may require dosage reductions or discontinuation of the oral agent. TZDs can be associated with weight gain, edema, and increased risk of congestive heart failure in combination with insulin. The insulin regimen to be prescribed and the exact treatment goals should be discussed with the patient.
Insulin-treated patients should be instructed in SMBG. When and how should glucose monitoring be used? Nevertheless, there are some patients for whom a simpler regimen is a reasonable compromise. When mealtime glucose control is needed or when glycemic goals are not met on a basal insulin regimen plus oral agents or a GLP-1 receptor agonist, insulin therapy intensification to a basal-bolus regimen using a rapid-acting insulin analog or inhaled insulin should be considered Table The incretins GLP-1 receptor agonists and DDP-4 inhibitors have properties similar to those of pramlintide and also increase endogenous insulin secretion.
The combination of basal insulin and incretin therapy decreases basal glucose and PPG and may minimize weight gain and the risk of hypoglycemia compared with basal-bolus insulin regimens. The frequency of hypoglycemia increases with intensive insulin targets, use of sulfonylureas, decreased caloric intake, delayed meals, exercise, alcohol consumption, CKD, T2D duration, and cognitive impairment [EL 4; NE]. Large randomized trials conducted in subjects with established T2D have revealed that subjects with a history of 1 or more severe hypoglycemic events had an approximately two- to fourfold higher rate of mortality for reasons that remain unknown 64 [EL 3; SS]; [EL 1; RCT].
It has been proposed that hypoglycemia may be a marker for persons at higher risk of death rather than being its proximate cause [EL 4; NE] ; nevertheless, avoidance of hypoglycemia by appropriately reducing insulin dosages seems prudent. Patients receiving insulin gain about 1 to 3 kg more weight than they do with other treatment agents. Physiologic insulin regimens, using both basal and prandial insulin, provided by either MDI or CSII, have not been formally tested in RCTs against nonphysiologic insulin regimens once or twice daily insulin.
Rather, physiologic insulin regimens have been formally studied as 1 component of a comprehensive treatment strategy for patients with T1D. Numerous RCTs have compared basal insulin analogs with NPH insulin in addition to rapid-acting analogs with regular human insulin. With insulin analogs, no additional improvements in A1C have been shown, but there is a consistent reduction of moderate and severe hypoglycemia [EL 4; review NE].
The starting dose of insulin is usually based on weight, with doses ranging from 0. No data support the superiority of 2 injections of a basal insulin analog over 1injection of basal insulin analog in patients with T1D. The dose of prandial insulin is usually determined by estimating the carbohydrate content of the meal. C ratios usually range from 1: Although various formulas have been used to estimate the appropriate ISF, this parameter should only be viewed as an estimation due to numerous factors that can alter blood glucose.
The most commonly used formula is: For most subcutaneous injections, this ranges from 4 to 6 hours. With the knowledge of the I: This is significantly simpler with CSII, as most pumps include bolus calculators to perform the calculations by pressing a few buttons. For those using MDI, there are a variety of smart phone apps available, in addition to several blood glucose meters that can assist patients with these calculations.
The amylin analog pramlintide, the only other medication approved for the treatment of T1D, is administered with prandial insulin. A1C reductions are consistently modest, and mild weight loss is common. Nausea is a common adverse effect. Tachyphylaxis is often seen after several years of therapy. While there is growing interest and anecdotal reports of successful use of both GLP-1 receptor agonists and SGLT2 inhibitors in T1D, to date appropriate trials have not been published, and formal recommendations cannot be provided.
In addition, recommendations for the use of metformin in T1D cannot be made due to lack of indication and concerns of lactic acidosis in a population predisposed to ketoacidosis. The classical definition of hypoglycemia in patients with DM is a low blood glucose level accompanied by symptoms of hypoglycemia e.
In addition, hypoglycemia symptoms can occur in the normal glucose range in a patient with very high glucose levels that drop quickly. SMBG can be helpful but is not necessarily diagnostic because of glucose meter inaccuracy. Severe hypoglycemia is defined as any low blood glucose event that requires assistance from another person to administer carbohydrates or glucagon or take other corrective action [EL 4; NE].
Certain hypoglycemia-related responses psychomotor function are altered in the elderly compared with younger patients. Although severe hypoglycemia generally results in recognizable symptoms, mild-to-moderate hypoglycemia may remain asymptomatic and unreported in patients with T2D or with hypoglycemia unawareness [EL 4; NE]. The primary cause of hypoglycemia is intensification of therapy to achieve a lower A1C target, as demonstrated by intensive therapy trials. The risk of hypoglycemia is greater in older patients and those with longer DM duration, kidney failure, or lesser insulin reserve.
The failure to recognize symptoms of hypoglycemia can increase the risk of subsequent hypoglycemia by causing autonomic failure, leading to a cycle of recurrent hypoglycemia and hypoglycemia unawareness [EL 4; NE]. Recent studies have suggested an association of hypoglycemia with adverse cardiovascular events. In ACCORD, hypoglycemia was considered a suspect behind the increased mortality observed in the intensive-treatment arm.
Moreover, the HR for hypoglycemia-related mortality was even higher in the standard therapy arm of that study adjusted HR in intensive treatment arm: A recent meta-analysis of prospective and retrospective clinical trials demonstrated that severe hypoglycemia doubled the risk of cardiovascular events [EL 2; MNRCT] , while an observational trial showed that, over a period of 5 years, mortality was 3.
The proposed mechanism for these effects posits that hypoglycemia reduces baroreceptor sensitivity and increases sympathoadrenal system activity, which can trigger a fatal ventriculararrhythmia in the setting of reduced baroreflex sensitivity [EL 4; NE]. Other short- and long-term consequences of severe hypoglycemia include neurologic conditions ranging from temporary cognitive impairment to dementia as well as major vascular events such as stroke, myocardial infarction, acute cardiac failure, ventricular arrhythmias, and sudden death [EL 4; NE]; [EL 4; NE]; [EL 4; NE].
The complications of hypoglycemia are also associated with short-term disability and higher healthcare costs [EL 4; NE]. Hypoglycemia is the primary limiting factor in the treatment of both T1D and T2D. It remains a significant barrier in terms of treatment adherence and achievement of glycemic goals [EL 4; NE]. Long-term management of hypoglycemia depends on appropriate adjustment of therapy to prevent hypoglycemia or reduce its frequency and severity in patients prone to hypoglycemia e.
In T2D, hypoglycemia typically occurs in association with use of exogenous insulin, sulfonylureas especially glyburide [EL 1; MRCT] , and glinides; symptoms may be mild, moderate, or severe. The risk of hypoglycemia may be further increased by the addition of other antihyperglycemic agents to sulfonylureas or insulin. Therefore, in adults with T2D, treatment strategies should emphasize classes of pharmaceutical agents that are not associated with severe hypoglycemia, many of which are available Table 9. Also, the role of hypoglycemia must be considered in determining ideal A1C goals for each patient.
SMBG is an important tactic to help patients document hypoglycemia, although it is essential that the glucose meter meet accuracy standards. Patients who have marked swings in glucose levels are particularly susceptible to hypoglycemia unawareness. The majority of persons with T2D either have uncontrolled hypertension or are on treatment for elevated blood pressure [EL 3; SS].
Hypertension is not only more prevalent in persons with T2D than in the general population, it also predicts progression to DM. Once diagnosed with hypertension, an individual is 2. The combination of hypertension and DM magnifies the risk of DM-related complications. Numerous other studies have also demonstrated decreased nephropathy and retinopathy progression. Once the diagnosis of hypertension is established, the data are clear that blood pressure lowering prevents both micro- and macrovascular complications associated with DM.
Analysis of the UKPDS data suggests that blood pressure lowering should be the first priority in managing a patient presenting with newly diagnosed hypertension and DM. While glucose and lipid management remain important, blood pressure lowering will have the greatest and most immediate impact on morbidity and mortality [EL 1; RCT]; [EL 1; RCT, questionnaires and other variables may have confounded]. Accurate measurement of blood pressure remains fundamental to the diagnosis and effective management of hypertension 8 [EL 4; NE]. The equipment, which can be aneroid, mercury, or electronic, should be inspected and validated on a regular maintenance schedule.
Initial training and regularly scheduled retraining in the standardized technique provides consistency in measurements. The patient must be properly prepared and positioned; blood pressure should be measured after being seated quietly for at least 5 minutes in a chair rather than on an exam table , with feet on the floor and arm supported at heart level. Caffeine, exercise, and smoking should be avoided for at least 30 minutes prior to measurement. Measurement of blood pressure in the standing position is indicated periodically, especially in those at risk for postural hypotension.
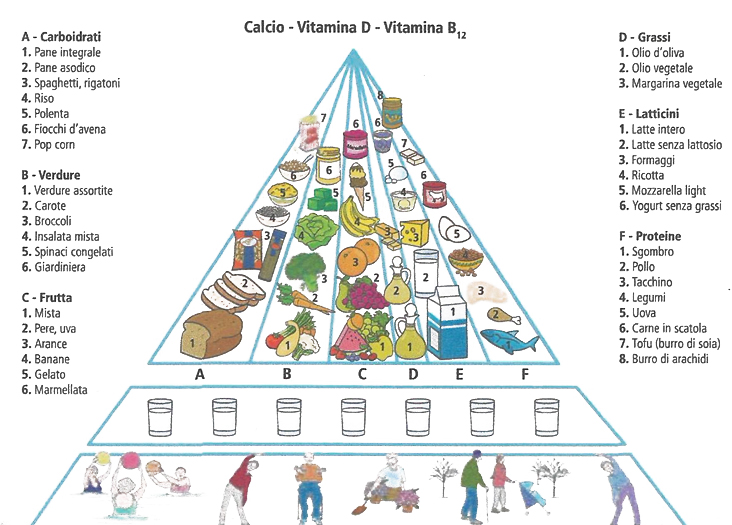
At least 2, and preferably 3, measurements should be made and the average recorded. While hour ambulatory blood pressure monitoring ABPM is not included as part of the diagnostic criteria for hypertension, it has become an important tool for guiding patient management. Routine use of ABPM, at least annually, should be considered for the evaluation of white coat hypertension, masked hypertension, and nighttime nondipping status, all of which are associated with increased long-term morbidity and mortality.
Blood pressure targets are based upon the combination of data from clinical trials and epidemiology studies and should be individualized for patients with consideration of their anticipated lifespan and risk factors for heart disease and stroke e. Frequent reassessment is needed to ensure that the blood pressure goal is maintained without unacceptable adverse effects.
The selection of medications can be guided by disease and ethnic-specific considerations. Whether any class is superior to another is no longer considered when choosing therapy because most patients with DM will need at least 2 to 4 drugs to achieve target blood pressure. The choice of pharmacologic agents is guided by additional considerations such as the presence of albuminuria, CVD, heart failure, or postmyocardial infarction status; possible metabolic side effects; number of pills per day; and cost.
Early in the disease process, the primary concerns will be slowing of nephropathy and retinopathy while minimizing impact on triglycerides Table As heart disease develops, consideration of cardiovascular benefits factor into the choice of agents for blood pressure lowering; given that diastolic heart disease develops early in T2D, the use of ARBs could be considered earlier, before the diagnosis of systolic heart failure.
However, the combination of multiple RAAS blockers i. The UKPDS study group performed a year post trialmonitoring observational study that demonstrated a loss of benefit within 2 years if tight blood pressure control was not maintained [EL 1; RCT, questionnaires and other variables may have confounded]. These data reinforce the imperative to initiate blood pressure-lowering therapy with continued reinforcement to maintain compliance with therapy. The introduction of fixed-dose combination tablets combining 2 or 3 agents in 1 pill has facilitated patient compliance and adherence with multidrug regimens and should be encouraged as part of initial therapy.
The use of multiple fixed-dose combination tablets can provide a 4-drug regimen with just 2 tablets, thus allowing a patient to reach their blood pressure goal while optimizing compliance with therapy. Risk stratification in this manner can guide management strategies. In prediabetes and DM, multiple disturbances in lipoprotein metabolism result from the combined effects of insulin deficiency, insulin resistance, and hyperglycemia. T2D dyslipidemia is characterized by increased levels of triglyceride-rich lipoproteins very low-density lipoprotein, intermediate-density lipoprotein, and remnant particles , low levels of HDL-C, and increased levels of small, dense LDL-P [EL 4; review NE].
Patients who have T1D with persistent proteinuria are at particularly increased risk of premature atherosclerosis [EL 4; NE]. However, the rising prevalence of overweight and obesity may contribute to increased rates of the lipid and lipoprotein pattern related to insulin resistance among prediabetic individuals and those with T2D [EL 1; RCT]. All patients should receive information about physical activity recommendations, a meal plan designed to improve glucose and lipids, and cardiovascular risk reduction strategies.
Lipids should be rechecked within 12 weeks. The combination of a statin with another lipid-lowering agent may be required to achieve these targets. In such patients, treatment should begin with therapeutic lifestyle changes for an initial 6- to 8-week trial. In patients younger than 40 years, initiation of statin therapy for primary prevention of CVD in both males and females needs to be individualized, based on other risk factors and comorbidities.
The use of various year or life-time risk calculators is an option to decide the intensity of treatment, but currently available risk calculators lack sufficient accuracy and are limited by discrepancies between predicted and observed event rates [EL 4; NE]; [EL 4; NE]. No study has yet been designed to investigate the cardiovascular outcomes benefit of adding bile acid sequestrants, niacin, or cholesterol absorption inhibitors to statins in patients whose atherogenic markers LDL-C, non-HDL-C, ApoB, and LDL-P are not already at target levels.
Such patients should be monitored closely to determine whether statin dose adjustment is necessary depending on comorbidities, drug interactions, and renal status [EL 4; NE]; [EL 4; NE]. Two separate RCTs tested the HDL-C-raising hypothesis in patients with coronary artery disease optimally treated with statins with or without ezetimibe.
However, in other settings, where the goals of these atherogenic markers have not been met, niacin remains a viable treatment option. The principles and goals of lipid management in prediabetes are the same as those for DM described previously Table 7. No randomized intervention trials dedicated to patients with prediabetes use ASCVD events as outcome measures.
Diet, exercise, and weight loss or maintenance should be emphasized for all prediabetes patients. Low HDL-C is also common in prediabetes. Niacin is effective in raising HDL-C, but it also increases insulin resistance and may accelerate the appearance of overt DM. Fibrates may be considered, but the use of gemfibrozil is discouraged owing to its interaction with statin clearance and the risk for severe rhabdomyolysis. Meta-analyses of statin RCTs indicate that statin use is associated with significant increases in the risk of progression to T2D among patients with prediabetes: Patients with prediabetes should be warned of the potential added risk of conversion to DM with statin use.
Diabetic nephropathy is represented histologically by the presence of basement membrane thickening, mesangial expansion, podocyte loss, and nodular or diffuse glomerulosclerosis [EL 4; NE]. The pathologic changes, which modestly correlate with the degree of kidney injury as measured by blood and urine tests, are typically present before functional tests are positive [EL 4; NE]. Consequently, prevention of microvascular complications such as nephropathy should be started upon diagnosis of DM and be intensified in those with evidence of kidney damage.
The AACE concurs with both guidelines in general. The KDIGO guidelines recommend phasing out the term microalbuminuria and replacing it with the term albuminuria. Testing for the presence of albuminuria can be done using a spot urine sample or a timed collection. Urinary albumin may be seen in the setting of urinary tract or systemic infection, after exercise, or in the presence of hematuria, so confirmation is necessary to establish the diagnosis of diabetic nephropathy.
Sudden onset or rapidly increasing AER should prompt additional tests to rule out other kidney diseases. Table 14 lists correlations between AER, urine dipstick, and tests of total protein excretion. Intensive glucose control has not been shown to diminish the progression of diabetic nephropathy or cardiovascular mortality in patients with advanced CKD, but these patients have an increased risk of hypoglycemia, so glycemic targets and therapies may need to be modified as diabetic nephropathy progresses.
How is hypertension managed in patients with diabetes? Patients with DM and CKD up to stage 4, including posttransplant patients, benefit from lipid lowering with statins. Slowing the progression of kidney dysfunction is critical for patient survival and quality of life. The RAAS-blocking drugs may potentiate hyperkalemia and may cause harm when used with nonsteroidal anti-inflammatory drugs NSAIDs or in patients with renovascular hypertension or dehydration.
They are not safe for use in pregnancy. Data on the use of aldosterone antagonists with ACE inhibitors or ARB classes is limited, but the same cautions apply. If the GFR continues to decline despite excellent glycemic and blood pressure control, protein restriction may be of some benefit. KDIGO recommends limiting protein intake to 0. Additional dietary restrictions may be required to control potassium and phosphorus levels.
Salt intake should be limited to 2 g per day in all patients with DM who require antihypertensive medications. Obesity is a risk factor for hypertension and incident CKD, so weight loss along with exercise is recommended for patients with DM without evidence of kidney disease as well as patients with category G2 to G4 CKD. Unintended weight loss is associated with poorer outcomes in dialysis patients.
Patients with CKD are at risk for drug toxicity and acute kidney injury. Antihyperglycemic therapies should be modified to reduce excessive drug exposure and hypoglycemia [EL 3; CSS]. Many other drugs should be avoided or used with caution in patients with CKD.
- Linee-guida e Raccomandazioni;
- BUY ON AMAZON'S NEVER EASY!
- Raising Godly Teens.
- Shadows Bloom (Tales of the Even).
- A little bit of BLACK MAGIC.
Patients should be informed of their CKD diagnosis and should avoid dehydration and imaging that requires gadolinium, high phosphate-containing bowel preparations, or high doses of iodinated contrast dyes. Patients with diabetic nephropathy should undergo annual or more frequent assessment of electrolytes to assess potassium and acid-base status; blood counts to assess anemia status; and calcium, phosphorus, vitamin D, and parathyroid hormone PTH measurements to assess mineral metabolism [EL 4; NE]. Hyperkalemia is managed by dietary restriction and adjustment of antihypertensive medications.
Iron given intravenously may produce better results than oral replacement. Active vitamin D preparations may be necessary to keep the PTH level from increasing as kidney function declines. Hyperphosphatemia should be corrected into the normal range with dietary modification and judicious use of phosphate binders. Referral to a nephrologist is appropriate when the presentation is atypical, progression of albuminuria or decline in eGFR is rapid, or when secondary manifestations of CKD require expert advice.
Referral of patients with stage 4 CKD to a nephrologist allows time for sufficient planning to accommodate individual patient needs [EL 4; opinion NE]. Renal transplantation is the preferred replacement therapy for patients with DM and ESRD because long-term outcomes are superior to those achieved with dialysis. For patients with T1D, the possibility of combined kidney-pancreas transplantation allows for considerably better outcomes [EL 2; PCS].
Diabetic retinopathy is the leading cause of blindness in adults. The lesions of diabetic retinopathy include background or nonproliferative retinopathy, macular edema, preproliferative retinopathy, and proliferative retinopathy. Higher levels of glucose and blood pressure, as well as the presence of nerve and renal diabetic complications, are associated with greater likelihood of developing retinopathy [EL 3; SS]. The goal is to detect clinically significant retinopathy before vision is threatened. Funduscopy performed by internists or endocrinologists is often suboptimal; therefore, referral to an experienced ophthalmologist for an annual dilated eye examination is recommended [EL 2; MNRCT].
The complete ophthalmologic examination can also detect other common conditions such as cataracts, glaucoma, and macular degeneration. The use of nonmydriatic fundus cameras equipped with digital transmission technology enables large-scale, POC screening for retinopathy [EL 3; SS]. Patients with abnormal retinal photographs are then triaged to full examination by an ophthalmologist.
This 2-step approach can be an efficient strategy for retinopathy screening at the population level, particularly in remote areas [EL 3; SS]. However, the system is still under development and does not replace the current recommendation for an annual dilated eye examination by an ophthalmologist from the time of diagnosis because of the lag between onset and diagnosis of T2D [EL 3; CSS]. As retinopathy develops over a period of 5 or more years from initial hyperglycemia, screening should be initiated within 5 years of diagnosis in patients with T1D [EL 3; SS].
Pregnancy is a risk factor for progression of retinopathy, and ophthalmologic examinations should be performed repeatedly during pregnancy and for 1 year postpartum [EL 2; PCS, longitudinal follow-up study]. Patients with active lesions may be followed up more frequently, while those who have had repeatedly normal eye findings can be seen less frequently. Good control of glycemia and blood pressure are also effective in slowing the progression of pre-existing background retinopathy. Research into other novel pharmacologic agents with potential benefits may lead to additional medical treatments [EL 1; RCT, small sample size].
Panretinal scatter laser photocoagulation is the treatment of choice for high-risk proliferative retinopathy [EL 4; review NE]. For macular edema, the combination of focal laser photocoagulation with intravitreal antivascular endothelial growth factor modalities appears to offer optimal benefit [EL 1; MRCT]. Vitrectomy is reserved for patients with persistent vitreous hemorrhage or significant vitreous scarring and debris [EL 4; review NE]. It is a major cause of falls in older patients that lead to lacerations, fractures, and traumatic brain injuries [EL 4; NE].
Diabetic neuropathy is a set of clinical syndromes that affect distinct regions of the nervous system, singly or in combination. It may be silent and go undetected while exercising its ravages, or it may present with clinical symptoms and signs that, although nonspecific and insidious with slow progression, also mimic those seen in many other diseases. Diabetic neuropathy is, therefore, diagnosed by exclusion.
Unfortunately neither endocrinologists nor nonendocrinologists have been trained to recognize the condition, and even when diabetic neuropathy is symptomatic, less than one-third of physicians recognize the cause or discuss this with their patients [EL 1; RCT]. Diabetic neuropathy encompasses multiple different disorders involving proximal, distal, somatic, and autonomic nerves. It may be acute and self-limiting or a chronic, indolent condition.
It may be focal such as a mononeuritis involving single nerves or entrapment neuropathies e. Proximal lumbosacral, thoracic, and cervical radiculoplexus neuropathies involving the proximal limb girdle are, for the most part, inflammatory demyelinating conditions requiring immunotherapy and, if caught early, are reversible [EL 4; NE]; [EL 4; review NE]; [EL 4; position NE]; [EL 4; NE].
They may be acute or chronic. Because of the lack of agreement on the definition and diagnostic assessment of neuropathy, several consensus conferences were convened to overcome the current problems. Several reviews discuss useful approaches to the treatment of the common forms of diabetic neuropathy, as well as algorithms for pain management, diagnosis, and treatment of the manifestations of autonomic neuropathy [EL 4; review NE]; [EL 4; review NE]. However, no treatments have been approved for the prevention or reversal of diabetic neuropathy.
Once large-fiber diabetic neuropathy has been diagnosed, therapy should be initiated to reduce symptoms and prevent further progression. It is vitally important to institute measures to prevent foot ulcers that lead to amputations. In general these are daily inspection, protective socks, appropriate footwear, and avoidance of injury. Patients with DM who have large-fiber neuropathies are uncoordinated and ataxic and are 17 times more likely to fall than their counterparts without neuropathy [EL 2; RCCS]. Low-impact activities that emphasize muscular strength and coordination and challenge the vestibular system such as a Bosu ball; use of rubber bands to strengthen lower limb muscles; and Pilates, yoga, and Tai Chi to strengthen the body core, may also be particularly helpful [EL 2; PCS, small sample size]; [EL 2; PCS, small sample size].
- The Soul of Science: Christian Faith and Natural Philosophy (Turning Point Christian Worldview Series)
- A Christmas Sermon (Annotated Edition)
- Golfs Simple Secrets - Increase Your Power
- Internet Cafe (Italian Edition)
- Divine Healing Hands: Experience Divine Power to Heal You, Animals, and Nature, and to Transform All Life (Soul Power)
- Lei do Bem - Lei nº 11.196/2005 (Portuguese Edition)